Estrogen receptor positive breast cancers are the most common type of breast cancer, characterized by tumor cells that grow in response to estrogen. Because these cancers rely on hormone signaling, treatments often focus on blocking estrogen activity or reducing hormone levels in the body.
Advances in hormone therapy, targeted treatments, and early detection have significantly improved outcomes for individuals diagnosed with ER positive breast cancer.
What Are Estrogen Receptor Positive Breast Cancers?
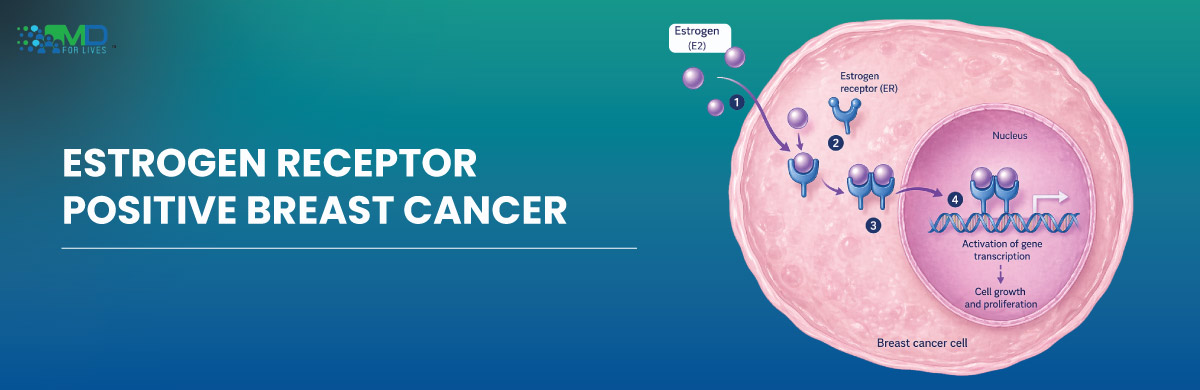
Estrogen receptor positive breast cancer refers to tumors that contain receptors that bind to the hormone estrogen.
When estrogen attaches to these receptors, it stimulates tumor cell growth.
Approximately 70 percent of breast cancers are hormone receptor positive, meaning they respond to estrogen or progesterone signaling.
These cancers are commonly referred to as ER positive breast cancer or hormone receptor positive breast cancer.
Because tumor growth depends on hormone signaling, treatments that block estrogen activity are highly effective.

Types of Hormone Receptor Positive Breast Cancer
Hormone receptor positive cancers are categorized based on which receptors are present.
ER-Positive Breast Cancer
Tumor cells contain receptors that respond to estrogen.
PR-Positive Breast Cancer
Tumor cells contain progesterone receptors.
ER and PR Positive Tumors
Many breast cancers contain both receptors and respond well to hormone therapy.
Hormone receptor status is determined through laboratory testing of biopsy samples.
Symptoms of Estrogen Receptor Positive Tumor
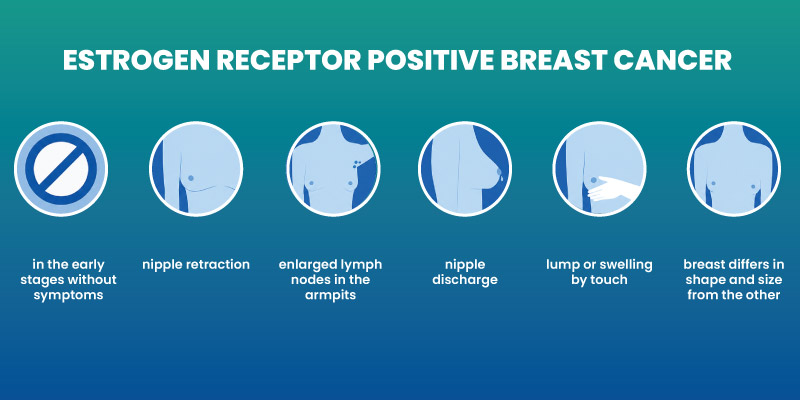
Early breast cancer often produces few symptoms, which is why routine screening is important.
Possible symptoms include:
- A lump in the breast or underarm
- Changes in breast shape or size
- Skin dimpling or thickening
- Nipple discharge
- Persistent breast pain
However, many cases are detected through mammography before symptoms appear.
What Causes Estrogen Receptor Positive Cancers?
The development of estrogen receptor positive cancers involves multiple biological and environmental factors.
Possible contributors include:
- Genetic mutations
- Hormonal exposure over time
- Age and reproductive history
- Family history of breast cancer
- Lifestyle factors such as obesity or alcohol use
Estrogen stimulates breast cell growth. When genetic mutations occur in these cells, uncontrolled growth may lead to cancer.
Read about does alcohol cause cancer
How Is ER Positive Breast Cancer Diagnosed?
Diagnosis usually involves several steps.
Imaging
Mammography, ultrasound, or MRI may identify suspicious breast lesions.
Biopsy
A biopsy removes tissue for laboratory examination.
Hormone Receptor Testing
Pathologists test tumor samples to determine whether the cancer is estrogen receptor positive.
This information guides treatment decisions.
Stages of Estrogen Receptor Positive Breast Cancer
Breast cancer staging describes how far the disease has progressed.
Stage 0
Non-invasive cancer confined to ducts.
Stage 1 and 2
Cancer is present in breast tissue and possibly nearby lymph nodes.
Stage 3
More extensive spread within regional lymph nodes.
Stage 4 Breast Cancer Estrogen Receptor Positive
Cancer has spread to distant organs such as bone, liver, or lungs.
Even at advanced stages, hormone therapy may slow disease progression.
ER Positive Breast Cancer Treatment Options
Treatment depends on stage, tumor characteristics, and patient health.
Common treatments include:
- Surgery
- Radiation therapy
- Hormone therapy
- Chemotherapy
For many patients, a combination of therapies is used to reduce recurrence risk.
Hormone Therapy for ER Positive Breast Cancer
Hormone therapy is the cornerstone of treatment for ER positive breast cancer.
These therapies block estrogen signaling or reduce estrogen production.
Common medications include:
Tamoxifen
Blocks estrogen receptors in breast tissue.
Aromatase Inhibitors
Reduce estrogen production in postmenopausal women.
Examples include anastrozole, letrozole, and exemestane.
Ovarian Suppression
In premenopausal women, medications or surgery may reduce estrogen production.
Hormone therapy may be prescribed for 5 to 10 years to lower recurrence risk.
Read about menopause hot flashes

Prognosis and Survival Rate
The prognosis for estrogen receptor positive breast cancer is generally favorable compared with other breast cancer types.
Key factors affecting survival include:
- Stage at diagnosis
- Tumor size and spread
- Response to therapy
- Overall health
Hormone receptor positive tumors often grow more slowly and respond well to endocrine therapy.
Can Estrogen Receptor Positive Breast Cancer Spread?
Yes. Like other cancers, ER positive breast cancer can metastasize.
Common sites of spread include:
- Bones
- Liver
- Lungs
- Brain
However, targeted therapies and hormone treatments have improved long-term control of metastatic disease.
Living With Estrogen Receptor Positive Breast Cancer
Managing breast cancer involves both medical treatment and supportive care.
Important aspects include:
- Regular follow-up appointments
- Monitoring for recurrence
- Maintaining healthy lifestyle habits
- Emotional and psychological support
Many patients continue normal daily activities during treatment and recovery.
New and Emerging Treatments
Research continues to improve treatment options for estrogen receptor positive breast cancers.
New approaches include:
- CDK4/6 inhibitors that slow tumor growth
- PI3K inhibitors for specific genetic mutations
- Personalized treatment strategies based on tumor biology
These advances are helping extend survival and improve quality of life.
Conclusion
Estrogen receptor positive breast cancers are the most common form of breast cancer and often respond well to hormone-based therapies. Early detection, accurate diagnosis, and targeted treatment strategies significantly improve outcomes.
Continued research into tumor biology and new therapeutic approaches is further advancing care for patients with ER positive breast cancer.
Frequently Asked Questions
Can ER positive breast cancer be cured?
Many cases diagnosed at early stages can be treated successfully with surgery, radiation, and hormone therapy. Long-term monitoring is important because recurrence can occur years after treatment.
Is ER positive breast cancer aggressive?
ER positive tumors typically grow more slowly than some other breast cancer types, although behavior can vary depending on stage and tumor biology.
Can ER positive breast cancer come back after treatment?
Yes. Recurrence can occur months or years after initial treatment, which is why hormone therapy and long-term follow-up are often recommended.
How long does ER positive breast cancer take to recur?
Recurrence risk can persist for many years. Some ER positive cancers may recur even after five to ten years, particularly without hormone therapy.
What foods are helpful or harmful for ER positive breast cancer patients?
Balanced diets rich in vegetables, fruits, whole grains, and healthy fats are generally recommended. Limiting alcohol and highly processed foods may help support overall health.

MDForLives is a global healthcare intelligence platform where real-world perspectives are transformed into validated insights. We bring together diverse healthcare experiences to discover, share, and shape the future of healthcare through data-backed understanding.