Lung cancer research studies are reshaping how the disease is detected, treated, and managed. Advances in molecular biology, targeted therapies, and clinical trials have significantly improved survival outcomes and expanded treatment options for patients with advanced lung cancer.
Over the past two decades, research lung cancer initiatives have shifted the focus from generalized treatment approaches to personalized medicine guided by tumor biology and biomarkers.
Lung Cancer Studies on Biological and Molecular Research
Modern lung cancer research increasingly focuses on the biological mechanisms that drive tumor growth.
Scientists are studying how genetic mutations, signaling pathways, and tumor microenvironments influence cancer development.
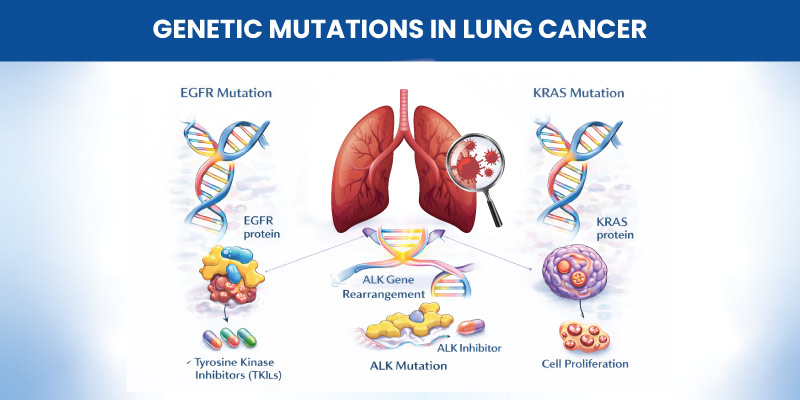
Key discoveries include mutations in genes such as:
- EGFR
- ALK
- KRAS
- ROS1
Understanding these molecular drivers allows clinicians to select therapies tailored to specific tumor characteristics.
Research on Biomarker Discovery and Validation
Biomarkers play a critical role in guiding treatment decisions in lung cancer.
Research studies have identified biomarkers that predict response to targeted therapies and immunotherapy.
Examples include:
- PD-L1 expression for immunotherapy selection
- EGFR mutations for targeted therapy
- ALK rearrangements guiding precision medicine treatments
Biomarker research continues to refine treatment strategies and improve patient selection for therapies.
Etiology, Risk Factors, and Prevention Research
Understanding the causes of lung cancer remains a major research focus.
Smoking is the most significant risk factor, but researchers also study additional contributors such as:
- Environmental pollution
- Occupational exposures
- Genetic susceptibility
- Secondhand smoke exposure
Prevention research aims to identify high-risk populations and develop strategies to reduce disease incidence.
Lung Cancer Research for Early Diagnosis and Screening
Early detection significantly improves survival outcomes.
Research has shown that low-dose CT screening can detect lung cancer at earlier stages among high-risk individuals.
Screening programs target people with:
- long smoking history
- older age
- increased risk factors
Advances in imaging technologies and biomarker testing are expected to further improve early detection.

Therapeutic Lung Cancer Research and Treatment Development
Major progress in lung cancer treatment advances has emerged from ongoing research.
Key treatment approaches include:
Drugs designed to attack specific genetic mutations have transformed care for many patients with advanced lung cancer.
Immunotherapy
Immune checkpoint inhibitors stimulate the immune system to recognize and destroy cancer cells.
Combination Therapy
Clinical research increasingly evaluates combinations of targeted therapy, immunotherapy, and chemotherapy to improve outcomes.
These strategies continue to expand options for advanced lung cancer treatment.
Lung Cancer Clinical Trials and Evidence Generation
Clinical trials remain essential for developing new therapies.
Lung cancer clinical trials evaluate new drugs, treatment combinations, and innovative approaches.
These trials help researchers determine:
- treatment effectiveness
- safety profiles
- optimal treatment sequences
Participation in clinical trials also gives patients access to emerging therapies before they become widely available.

Research Studies on Supportive Care and Survivorship
In addition to treatment development, researchers are studying supportive care strategies for lung cancer patients.
Areas of focus include:
- symptom management
- treatment side effects
- rehabilitation and survivorship programs
These studies aim to improve quality of life during and after treatment.
Patient Outcomes, Symptom Management, and Quality of Life
Patient-centered research examines how treatments affect daily functioning and overall well-being.
Common symptoms that researchers address include:
- fatigue
- breathlessness
- chronic cough
- pain
Improving symptom control remains an important part of lung cancer management.
Real-World Evidence and Comparative Effectiveness Research
Clinical trials provide valuable evidence, but researchers increasingly rely on real-world data to understand how treatments perform outside controlled study settings.
Real-world research helps evaluate:
- treatment effectiveness in diverse populations
- long-term outcomes
- healthcare resource utilization
These insights guide treatment decisions and policy development.
Read also about Phage Therapy
Emerging Research in Lung Cancer Management
Several emerging areas are shaping the future of lung cancer research.
These include:
- liquid biopsy for early detection
- artificial intelligence in imaging analysis
- personalized treatment strategies
- combination immunotherapy approaches
These innovations aim to improve survival and reduce treatment toxicity.
Read about Immunotherapy Side effects
Conclusion
Lung cancer research studies continue to transform clinical practice by advancing early detection, improving treatment options, and enhancing patient outcomes.
From biomarker discovery to large-scale clinical trials, ongoing research is expanding understanding of the disease and enabling more precise treatment strategies. Continued investment in lung cancer research will be essential for improving survival and quality of life for patients worldwide.
Read also about Precision medicine
Frequently Asked Questions
What are the latest advances in early detection and lung cancer screening research?
Recent studies focus on improving low-dose CT screening and developing blood-based biomarkers that may detect lung cancer earlier than imaging alone.
What are the major challenges in current lung cancer clinical trials?
Challenges include patient recruitment, identifying appropriate biomarkers for therapy selection, and ensuring trial results apply to real-world patient populations.
How generalizable are practice-changing lung cancer trials to real-world populations?
Some trials enroll carefully selected patients, which may limit generalizability. Real-world studies help confirm whether treatments remain effective across broader patient groups.

MDForLives is a global healthcare intelligence platform where real-world perspectives are transformed into validated insights. We bring together diverse healthcare experiences to discover, share, and shape the future of healthcare through data-backed understanding.