
Over the past five years up to 2022, IBISWorld estimates that the obesity rate among adults aged 18 and older has increased an annualized 1.8% to 33.0 people per 100 individuals. The prevalence of diabetes in adults worldwide was estimated to be 4.0% in 1995 and to rise to 5.4% by the year 2025. It is higher in developed than in developing countries. The global diabetes prevalence in 2019 was estimated at 9.3% (463 million people), rising to 10.2% (578 million) by 2030, and 10.9% (700 million) by 2045 (P.Saeedi et.al IDF Diabetes Atlas Committee. 2019).
This appears less like behavior, and more exposure, as grave as any pandemic, COVID-19, influenza, typhoid, etc., a microbial phenomenon.
Research from Kings College and University of Gottingen (J.Davis et.al, Centre for Global health, 2018). The global cost of diabetes is set to almost double to $2.5 trillion by 2030, suggesting that even if countries meet internationally set targets, the global economic burden from the disease will still increase by 88%. A study in 2013 by the Government Accountability Office claimed Medicare would be “broke” by 2026, which is not quite the case, but the fact society has not done anything during this period to mitigate this potential catastrophe is concerning.
Why is there no call to arms against this? Where are the pharma investments, the government outcries, and the communion of people? Why has this not become a public health crisis?
Below you can see a slide that demonstrates the phenomenon. Two equally weighted adult men, which one is healthy, and which one is sick?
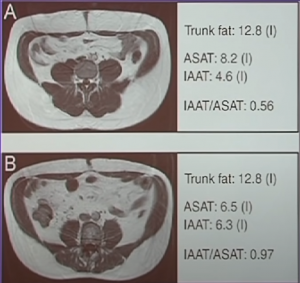
Aspartate aminotransferase (ASAT), intra-abdominal adipose tissue (IAAT)
The answer is the one on the bottom (B) is actually sick. You can see more visceral fat surrounding the organs. Though (A) has “love handles”, he is still perfectly healthy because subcutaneous fat is good for you. (S. Porter et.al “Abdominal Subcutaneous Adipose Tissue: A Protective Fat Depot?” Jun 2009).
How do you know how fat you are? Standing on a scale does not tell you this. You can start with waist circumference, and laboratory tests will confirm. And if you are of normal weight, does this mean you will not get dyslipidemia or hypertension? Not exactly, everybody is at risk. Because everybody is exposed. And what are they exposed to? Obesity is not the problem, despite what all the newspapers, magazines, government websites, social media, health boards, etc., want you to think.
Metabolic syndrome is the problem.
Metabolic syndrome covers 75% of all health care costs today. They incorporate diabetes, hypertension, lipid abnormalities, cardiovascular disease, non-alcoholic fatty liver disease, polycystic ovarian disease, dementia, and cancer.
The most common interpretation of obesity is: “If you eat it, you better burn it, or you’re going to store it”
People to this day believe that obesity is the result of two behaviors that you are not controlling: calories in (eating too much) and calories out (not burning it off). The dogma suggests that a calorie is a calorie, and the corollary of this is a person is getting obese, either through free will, lack of personal responsibility, gluttony and sloth, and lack of diet and exercise.
The fiction suggests obese people are to blame for not controlling themselves.

Are food companies helping obese people?
Take a look below, and make your own mind up about what you see:
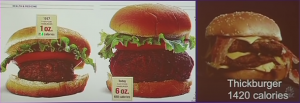
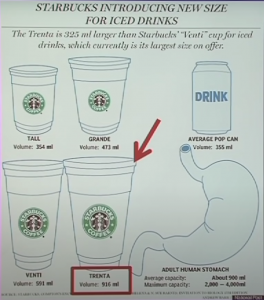
“Well we don’t force you to eat!” Fast-food industries can claim, as they make portions bigger, charge extra for these portions, and emphasize to employees to “sell” the larger meal option to the consumer.
Is it down to income?
Do poor people have less access to exercise equipment or healthy foods? In every high street, especially in poorer towns in the UK, you will see an array of fast-food restaurants or cafes with stodgy sandwiches and fatty beverages and of course pubs and gambling places. It is as if the government has resigned itself to throwing their people under the bus.
How about the activity? Are obese people just lazy, unhappy, and unwilling to put aside some time to exercise, despite the thousands of articles stressing the importance of walking, running, and keeping fit?
Below is a study conducted by Kimm et al. in NEJM 2002, showing a graph of age vs metabolic equivalent of task (the amount of energy used, with 1.3 MET the amount of energy we use while sitting down, reading, and running = 8-9 MET). The line at the top was ‘white girls’ (females from Caucasian backgrounds) and the line at the bottom ‘black girls’ (African American females).
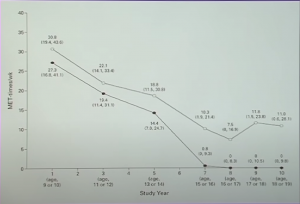
By age 15-18 the ‘black girls’ showed a stark lack of movement. This data was spread through numerous articles, making newspaper headlines throughout the world. They used it to fit a polemic: “black women don’t do anything, they eat a lot, that’s why they get diabetes and are obese”. Of course, this is all hyper-exaggeration and serves little purpose but to scare and insult a race to sell copy and get tongues wagging. The study size was clearly not conclusive for a whole race of people. It told a story but did not tell the truth.
No child chooses to be obese. The quality of life of an obese child is equivalent to those on cancer chemotherapy (Schwimmer et.al, JAMA 2009)
Is it the parent’s fault then?
In April 2015, Adrian Balog, from Manchester, England, a morbidly obese 13 year old needed a heart transplant. However, as a result of his diet, suffered heparin-induced thrombocytopenia (blood disorder causing clots), meaning he was ineligible for surgery. He died shortly after.
“Adrian was never taught how to eat healthily and had no contact with weight management services in his short life,” said his coroner Zak Golombeck. Cue social media, taking his parents to town over their lack of responsibility.
Do you think the parents should be blamed? Did their lack of responsibility cause their child to die?
In part 2, we will discuss diets and who or what really is to blame for the global obesity crisis?

MDForLives is a global healthcare intelligence platform where real-world perspectives are transformed into validated insights. We bring together diverse healthcare experiences to discover, share, and shape the future of healthcare through data-backed understanding.




