PSMA PET scan for prostate cancer has emerged as one of the most precise imaging tools for detecting and staging disease. By targeting prostate-specific membrane antigen expressed on tumor cells, PSMA PET CT scan enables earlier identification of metastatic spread compared to conventional imaging. Recent studies have demonstrated its impact on treatment decisions, recurrence detection, and long-term management strategies. As precision oncology advances, PSMA PET imaging is redefining diagnostic pathways in prostate cancer care.
What is prostate-specific membrane antigen PET? (PSMA PET Scan)
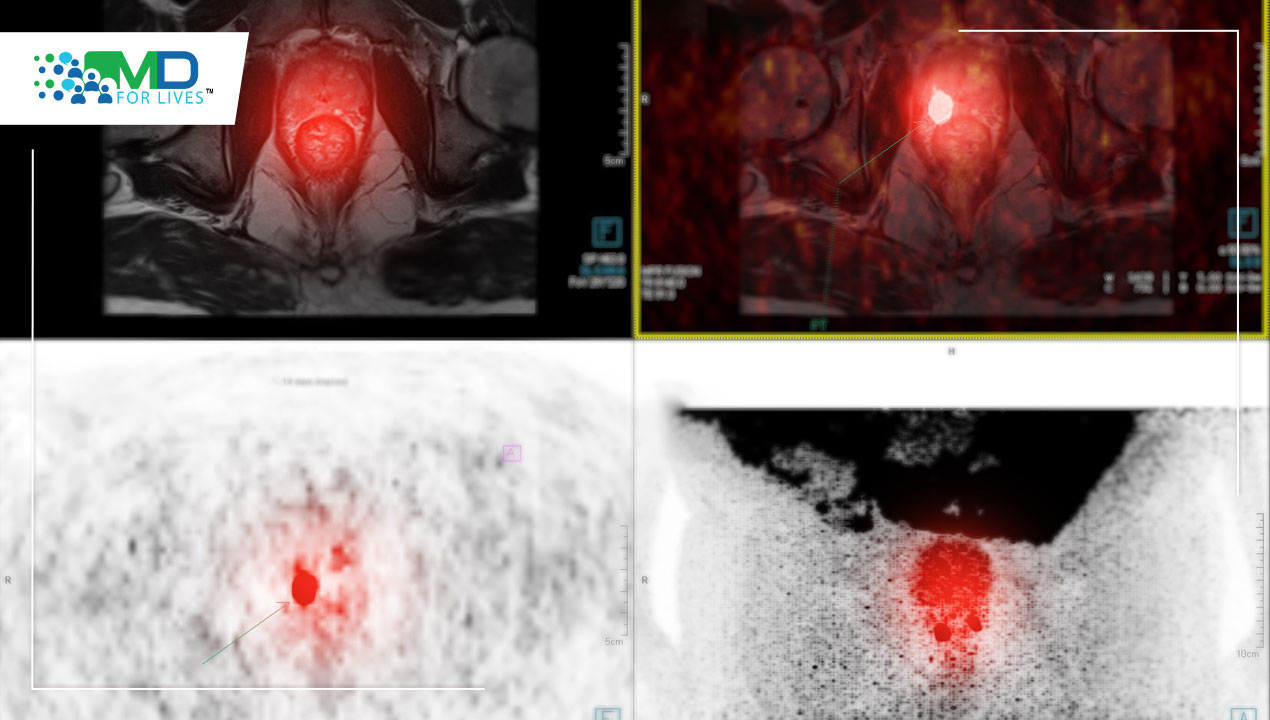
A PSMA PET scan is a nuclear medicine imaging technique that uses a radiotracer targeting prostate-specific membrane antigen, a protein overexpressed in most prostate cancer cells.
The PSMA PET scan full form refers to Prostate-Specific Membrane Antigen Positron Emission Tomography. When combined with CT, it is known as a PSMA PET CT scan, integrating metabolic and anatomical imaging for greater diagnostic clarity.
Unlike conventional PET scans that rely on glucose metabolism, PSMA-targeted tracers such as Gallium-68 or Fluorine-18 bind directly to cancer-associated cell surface proteins, improving specificity.
How does PSMA PET work?
The scan involves injecting a small amount of radioactive tracer that binds selectively to PSMA-expressing cells. Once attached, the tracer emits signals detected by PET imaging systems.
This enables:
- · Detection of lymph node metastases
- · Identification of bone lesions
- · Localization of recurrent disease at low PSA levels
- · Evaluation of treatment response
By targeting molecular expression rather than structural changes alone, PSMA PET imaging improves early detection sensitivity.
How is PSMA PET imaging different from current prostate cancer imaging?
Traditional imaging methods include CT scans, MRI, and bone scans. These rely primarily on structural changes.
PSMA PET scan prostate cancer imaging differs in three ways:
1. Molecular targeting of cancer-specific protein
2. Higher detection rates at low PSA levels
3. Improved identification of micro-metastatic disease
A landmark trial published in 2020 demonstrated significantly higher accuracy of PSMA PET compared to conventional imaging in high-risk prostate cancer staging. This has influenced guideline discussions globally.
Duration – How long does a PSMA PET Scan take?
Patients frequently ask, how long does a PSMA PET scan take?
The total time is approximately 2 to 3 hours:
- Radiotracer injection
- Waiting period of 45 to 60 minutes
- Imaging session lasting 20 to 40 minutes
The scanning portion itself is typically under 30 minutes.
Procedure – How PSMA PET Scan Works?
The PSMA PET scan procedure follows a structured sequence:
1. Pre-scan evaluation
2. Intravenous tracer injection
3. Rest period for tracer uptake
4. Whole-body PET CT scan
5. Radiologist interpretation
Most patients experience minimal discomfort. The radiation exposure is within diagnostic safety standards.
What are the benefits of PSMA PET treatment?
Although PSMA PET is diagnostic rather than therapeutic, its clinical value influences treatment strategy.
Benefits include:
- More accurate staging
- Reduced unnecessary surgeries
- Targeted radiation planning
- Improved recurrence detection
- Informed systemic therapy decisions
In cases of biochemical recurrence, PSMA PET scan for prostate cancer can detect lesions even at PSA levels below 0.5 ng/mL.
Accuracy of PSMA PET Scan
Multiple studies report superior sensitivity and specificity compared to conventional imaging. Detection rates increase proportionally with PSA levels, yet remain meaningful even at low PSA thresholds.
Accuracy improvements have resulted in:
- Upstaging of previously localized disease
- Alteration of management plans in over 25 to 40 percent of cases in certain trials
- Enhanced identification of oligometastatic disease
This precision directly impacts long-term survival planning.
Who should consider PSMA PET?
PSMA PET is typically recommended for:
- High-risk newly diagnosed prostate cancer
- Biochemical recurrence after surgery or radiation
- Rising PSA with negative conventional imaging
- Evaluation before salvage therapy
Clinical eligibility depends on national regulatory approval and physician assessment.
What happens during the PSMA PET Scan?
Patients are positioned on a scanning table that moves through a ring-shaped PSMA PET scan machine. The scanner captures signals emitted by tracer-bound cells.
The experience is non-invasive and painless. Movement must be minimized to ensure image clarity.
PSMA PET Scan Preparation
PSMA PET scan preparation scan preparation is straightforward:
- Hydrate adequately
- Avoid strenuous activity before the scan
- Follow specific instructions regarding medications
- Fasting is generally not required unless advised
Patients should inform clinicians about allergies or medical conditions.
PSMA PET Scan Results
PSMA PET scan results are interpreted by nuclear medicine specialists. Reports indicate:
- Presence or absence of metastatic lesions
- Location and number of lesions
- SUV values indicating tracer uptake intensity
These findings guide next-step management.
PSMA PET Scan Side Effects
Patients often ask about side effects of PSMA PET scan procedures.
The procedure is generally well tolerated. Possible effects include:
- Mild injection site discomfort
- Rare allergic reaction
- Minimal radiation exposure
Serious adverse effects are uncommon.
Cost Considerations
Search interest in PSMA PET scan cost and how much does a PSMA PET scan cost continues to grow.
In the United States:
- Cost may range from $3,000 to $7,000
- Coverage varies by insurer
- Medicare coverage depends on clinical indication
Questions such as is PSMA PET scan covered by Medicare should be addressed directly with providers and insurers.
In the UK, PSMA PET scan UK access may depend on NHS commissioning policies.
Does PSMA PET Scan Detect Other Cancers?
Although primarily used in prostate cancer, PSMA expression has been observed in some other tumor types. However, its validated clinical application remains centered on prostate malignancy.
Treatment After PSMA PET Scan
Treatment after the scan depends on findings:
- Localized disease may lead to surgery or radiation
- Oligometastatic disease may prompt targeted therapy
- Widespread metastasis may require systemic treatment
The scan functions as a decision-support tool within multidisciplinary oncology planning.
The Future of PSMA PET-CT – How PSMA Revolutionizes Staging for Prostate Cancer?
The future direction includes:
- Integration with AI-based imaging analysis
- Radioligand therapy using PSMA-targeted agents
- Earlier detection thresholds
- Personalized treatment mapping
Emerging studies continue to evaluate survival benefits associated with PSMA-guided management strategies.
Conclusion
The PSMA PET scan represents a significant advancement in prostate cancer imaging. By combining molecular targeting with high-resolution imaging, it improves staging precision, recurrence detection, and therapeutic planning. As research expands and access broadens, PSMA PET CT scan technology is expected to become integral to personalized prostate cancer care pathways.
Healthcare intelligence continues to evolve as imaging, data, and clinical insight converge.
Discover how global healthcare professionals are shaping oncology intelligence. Visit MDforlives.
Frequently Asked Questions
What is PSMA in PET scan?
PSMA stands for Prostate-Specific Membrane Antigen, a protein expressed on prostate cancer cells that is targeted during imaging to detect tumor presence.
At what PSA level should a PSMA scan be done?
PSMA scans may detect disease even at PSA levels below 0.5 ng/mL, though detection rates increase with higher PSA values. Clinical context determines timing.
How much does a PSMA PET scan cost in the US?
Costs typically range between $3,000 and $7,000 depending on facility, tracer type, and insurance coverage.
What is the difference between a PSMA PET scan and a regular PET scan?
A regular PET scan often uses FDG tracer targeting glucose metabolism, whereas PSMA PET specifically binds to prostate cancer cell surface proteins, increasing specificity.
How to prepare for a PSMA PET Scan?
Hydration is recommended. Specific preparation instructions are provided by the imaging center.
What to Expect from a PSMA PET Scan?
Patients can expect tracer injection, a waiting period for uptake, and a painless scanning session lasting under an hour.

MDForLives is a global healthcare intelligence platform where real-world perspectives are transformed into validated insights. We bring together diverse healthcare experiences to discover, share, and shape the future of healthcare through data-backed understanding.




