AI in endoscopy has already entered the procedure room. But has it earned a seat in the decision?
That is the question now shaping gastroenterology practice. Artificial intelligence is increasingly visible in real-time endoscopic workflows, especially through computer-aided detection tools for colonoscopy and lesion recognition. Its promise is clear: support endoscopists, improve detection, reduce variability, and help clinicians see what may otherwise be missed.
Yet the real-world story is more cautious.
Recent clinical guidance and expert consensus have recognized AI’s potential in gastrointestinal endoscopy, particularly in detection-oriented tasks. At the same time, leading societies continue to highlight evidence gaps around long-term outcomes, workflow integration, governance, cost, and the clinical meaning of what AI detects. In other words, AI may be helping endoscopists see more. The harder question is whether it is helping them decide differently.
An MDForLives survey among gastroenterologists and interventional endoscopists reflects this exact tension. AI adoption is no longer the main issue. Trust in real-time decision influence is.
AI Is Being Used, but Not Yet Standardized
The MDForLives findings show that 68.6% of clinicians report using AI either routinely or selectively in endoscopic practice. Usage is evenly split, with 34.3% reporting routine integration and another 34.3% using AI selectively. Only 17.1% say they are not currently using AI.
This suggests that AI has moved beyond early curiosity. It is now part of many clinical environments.
But the split between routine and selective use is important. It shows that AI adoption is not yet standardized across endoscopy. Some clinicians may use AI as a regular procedural layer, while others activate it only in selected cases or settings where its value feels clearer.
This is not resistance. It is controlled adoption.
Clinicians appear to be asking a practical question: where does AI genuinely improve the procedure, and where does it simply add another interpretive layer?
Colonoscopy Remains the Clearest Value Zone
When clinicians were asked where AI adds the greatest value today, colonoscopy stood out clearly. 57.1% identified colonoscopy, particularly polyp detection and characterization, as the strongest area of benefit.
That aligns with the broader evidence environment. AI in endoscopy has advanced most visibly through computer-aided detection, especially for colorectal polyp and adenoma detection. The clinical logic is easy to understand. Colonoscopy involves visual scanning, repeated pattern recognition, and detection-sensitive quality metrics. These are areas where AI can add support without immediately replacing clinical judgment.
But the concentration of value in colonoscopy also says something else: AI’s impact is not yet evenly distributed across all endoscopic procedures.
Applications in EUS, upper GI endoscopy, and IBD surveillance may be promising, but they appear less mature in clinician perception. This matters because AI in endoscopy cannot be judged as one category. Detection in colonoscopy, lesion characterization, risk assessment, and follow-up planning are very different clinical tasks.
Trust does not transfer automatically from one task to another.
Detection Support Is Not the Same as Decision Authority

The survey shows a clear benefit signal around detection. 34.3% of clinicians said AI has improved lesion detection, while 25.7% reported increased diagnostic confidence.
But decision influence remains much more limited. Only 14.3% said AI frequently influences real-time clinical decisions during procedures. Another 40.0% said it occasionally informs decisions, while 25.7% said it rarely affects decisions.
This gap is the strongest insight in the data.
AI is present. It is useful. It may improve visibility. But it is not yet decisive for most clinicians.
That distinction matters deeply in endoscopy. A system that flags a lesion is assisting detection. A system that shapes whether to resect, biopsy, characterize, escalate, or alter follow-up is influencing clinical responsibility.
Clinicians appear comfortable with AI as a second observer. They are far more cautious about AI as a decision-shaping partner.
This balance reflects the broader debate around AI vs Human decision-making in healthcare, where the greatest value often comes from combining AI-driven insights with clinician expertise rather than replacing clinical judgment.
Reliability Defines the Ceiling of Trust
Reliability is where the clinical hesitation becomes visible. Only 8.6% of clinicians described AI-assisted differentiation between neoplastic and non-neoplastic lesions as highly reliable. A majority, 54.3%, described it as moderately reliable. A combined 37.1% reported limited or insufficient reliability.
In many areas of healthcare, “moderately reliable” may sound encouraging. In real-time endoscopy, it is more complicated.
Procedural decisions are immediate. A lesion must be interpreted in context. The endoscopist remains accountable. If AI output is only moderately reliable, it may not reduce cognitive load. It may add verification work.
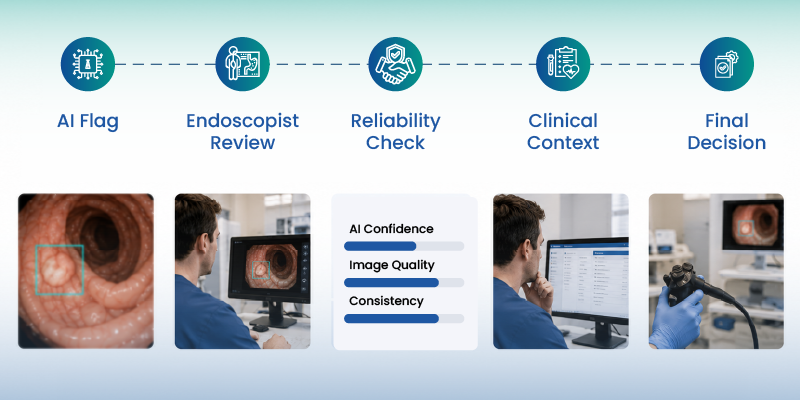
This is why moderate reliability can create a hidden burden. The clinician must notice the AI signal, assess whether it fits the endoscopic view, compare it with clinical context, and decide whether it changes action. AI may reduce the chance of missing something, but it may also increase the need to confirm.
The result is not full delegation. It is supervised assistance.
Adoption Barriers Are Structural, Not Just Technical
When clinicians identified the main limits to broader AI adoption, cost or reimbursement led at 31.4%, followed by integration with existing systems at 25.7% and trust in outputs at 17.1%.
This pattern shows that the challenge is not only algorithm performance. It is the operating environment around the algorithm.
This reflects a broader shift toward smart hospital technology, where the success of AI depends not only on algorithm accuracy but also on how effectively digital systems, workflows, and clinical infrastructure work together.
An AI tool may perform well in a study, but clinical value depends on whether it fits existing systems, supports documentation, avoids workflow disruption, has a sustainable payment model, and gives outputs clinicians can explain and trust.
For endoscopy units, this matters because procedural efficiency is already tightly managed. If AI adds friction, requires parallel verification, or creates uncertainty around documentation and accountability, adoption may remain uneven even when clinicians see potential benefit.
The future of AI in endoscopy will depend as much on implementation design as algorithm accuracy.
Clinicians Are Still Protecting the Boundary of Judgment
The survey suggests that gastroenterologists are not rejecting AI. They are defining its boundaries.
AI is more trusted for detection than interpretation. It is more accepted as an assistive layer than a decision authority. The strongest hesitation appears around higher-stakes areas such as lesion characterization, cancer-risk interpretation, resection decisions, biopsy decisions, and follow-up planning.
This is where the clinical line becomes clear.
Similar trust dynamics are emerging in AI for mental health, where clinicians are exploring how AI can support assessment and care delivery while maintaining human oversight for complex clinical decisions.
Endoscopists may welcome help in seeing more. But deciding what that finding means remains a clinician-held responsibility.
That boundary is likely to remain important even as AI improves. In real-time procedures, trust is not only about whether the system is correct. It is about whether the clinician can understand, validate, and defend the output at the point of care.
AI’s Future Looks Selective, Not Sudden
Looking ahead, clinicians expect AI adoption to expand, but cautiously. 48.6% believe adoption will expand selectively over the next 2 to 3 years, while 22.9% expect it to become standard of care. At the same time, 42.9% believe AI may become decision-shaping, but only with safeguards.
That is a measured outlook. It reflects interest without overconfidence.
A similar pattern can be seen with GLP-1 therapy in obesity care, where strong clinical potential has been accompanied by ongoing questions around access, long-term adherence, real-world outcomes, and sustainable integration into routine practice.
AI in endoscopy is likely to grow first where the use case is clearest: detection support, quality improvement, documentation assistance, workflow support, and selected procedural guidance. Broader decision-shaping roles will require stronger evidence, reliability, workflow integration, governance, and clarity around responsibility.
The direction is forward. The pace is conditional.
Closing Perspective
AI in endoscopy is not failing. It is entering its trust-building phase.
The MDForLives findings show that clinicians already recognize its value, especially in colonoscopy and lesion detection. But they also reveal that adoption and trust are not the same thing.
AI can be used without being fully relied upon. It can improve detection without controlling decisions. It can support confidence without replacing clinical judgment.
That is the real-world position of AI in endoscopy today: clinically useful, increasingly adopted, but still bounded by trust.
The next stage will not be defined by whether AI can see more. It will be defined by whether clinicians can trust it enough to decide differently when it matters.
Looking ahead, clinicians expect AI adoption to expand, but cautiously. 48.6% believe adoption will expand selectively over the next 2 to 3 years, while 22.9% expect it to become standard of care. At the same time, 42.9% believe AI may become decision-shaping, but only with safeguards.
That is a measured outlook. It reflects interest without overconfidence.
AI in endoscopy is likely to grow first where the use case is clearest: detection support, quality improvement, documentation assistance, workflow support, and selected procedural guidance. Broader decision-shaping roles will require stronger evidence, reliability, workflow integration, governance, and clarity around responsibility.
The direction is forward. The pace is conditional.
FAQs:
How is AI currently used in endoscopy?
AI is most commonly used as a detection-support tool in endoscopy, especially during colonoscopy for polyp and lesion detection. Some clinicians use it routinely, while others apply it selectively.
Does AI improve adenoma or lesion detection in colonoscopy?
AI-assisted colonoscopy has shown value in improving detection-related outcomes, particularly for colorectal polyps and adenomas. However, clinical guidance still highlights uncertainty around long-term outcomes such as colorectal cancer incidence and mortality.
Why is clinician trust in AI-assisted endoscopy still limited?
Trust remains conditional because clinicians need consistent reliability, explainable outputs, workflow integration, governance, and clarity around clinical responsibility before AI can influence real-time decisions more strongly.
Is AI reliable enough to guide real-time endoscopic decisions?
In the MDForLives survey, most clinicians described AI-assisted differentiation as moderately reliable rather than highly reliable. This suggests AI is useful for support, but not yet trusted as an independent decision authority.
What limits broader AI adoption in endoscopy?
The leading barriers reported in the MDForLives survey include cost or reimbursement, integration with existing systems, and trust in AI outputs.
Will AI become standard of care in endoscopy?
Clinicians expect AI adoption to expand, but selectively. Many believe AI may become decision-shaping only with safeguards around reliability, governance, workflow integration, and accountability.

MDForLives is a global healthcare intelligence platform where real-world perspectives are transformed into validated insights. We bring together diverse healthcare experiences to discover, share, and shape the future of healthcare through data-backed understanding.