
A retinal scan is flagged by an AI system within seconds. The result suggests early pathology. The clinician pauses, reviews the image again, and only then decides what happens next.
That moment captures the real position of AI in ophthalmology today.
Artificial intelligence is no longer sitting outside clinical care as a future-facing idea. It is already entering ophthalmic imaging workflows, particularly in retinal screening, OCT interpretation, glaucoma assessment, and reporting support. Ophthalmology is naturally suited to AI because it relies heavily on high-resolution images, pattern recognition, longitudinal comparison, and early disease detection.
Yet the presence of AI does not automatically mean full clinical trust.
The MDForLives survey among ophthalmologists, retina specialists, and glaucoma specialists across North America and Western Europe shows a clear gap: 67% of clinicians report regular use of AI tools in ophthalmic imaging, but only 45% report full confidence in AI outputs.
That gap is the story. AI adoption is becoming operational. Clinical trust is still conditional.
AI Has Moved From Pilot to Practice
AI in ophthalmology has crossed an important threshold. It is no longer being discussed only as an innovation project. In many clinical environments, AI tools are already being used in screening, image analysis, early detection, and workflow support.
This fits the broader direction of ophthalmic care. AI-enabled devices and diagnostic systems have already reached regulated clinical use in selected areas, including diabetic retinopathy screening. The FDA’s authorization of an autonomous AI-based diagnostic system for detecting more than mild diabetic retinopathy marked an important signal that AI could move beyond research into clinical implementation.
But MDForLives data suggests that clinicians are not adopting AI uniformly across all types of decisions. They appear most comfortable using it where physician oversight remains central and where AI functions as a support layer rather than a decision authority.
This is not resistance to AI. It is selective trust.
This evolving balance between clinician expertise and algorithmic support reflects the broader discussion around AI vs Human in healthcare, where the question is increasingly about collaboration rather than replacement.
Where AI Adds Value: Earlier Detection and Imaging Support
The strongest value of AI in ophthalmology appears to sit in areas where pattern recognition is central. Retinal imaging, OCT interpretation, diabetic retinopathy screening, and glaucoma progression analysis all generate the kind of visual and longitudinal data that AI systems are built to analyze.
In these settings, AI can support earlier detection, improve consistency in image interpretation, and help clinicians manage growing screening and imaging volumes. For ophthalmic practices facing rising patient demand and limited specialist time, these benefits are meaningful.
Similar benefits are being observed with AI in endoscopy, where real-time image analysis is helping clinicians detect abnormalities earlier and improve procedural accuracy.
But the clinical role of AI remains bounded. Clinicians may welcome AI when it flags a possible abnormality, highlights progression risk, or supports reporting efficiency. They become more cautious when the output moves closer to diagnosis, treatment escalation, or patient management decisions.
The difference is important: AI may help clinicians see earlier, but it does not yet mean clinicians are ready to decide differently without verification.
The Trust Gap Is About Consistency, Not Just Accuracy
The MDForLives findings show that 58% of clinicians question the consistency of AI accuracy, while 49% express concern about over-reliance.
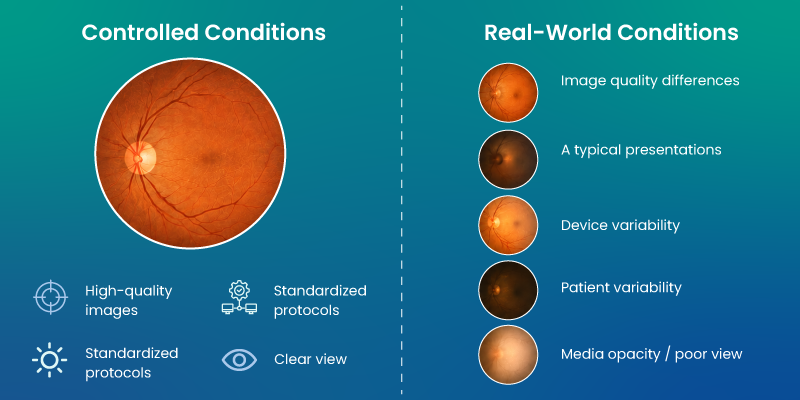
That distinction matters. Clinicians are not simply asking whether AI can perform well in ideal conditions. They are asking whether it can remain dependable across real-world variability.
Clinical imaging is rarely perfect. Image quality can vary. Patients may present atypically. Disease may overlap across conditions. Devices, acquisition methods, and patient populations may differ between sites. An AI system that performs well in controlled datasets may still need careful validation in everyday practice.
For ophthalmologists, this changes the trust equation.
A tool that is accurate sometimes can be useful. A tool that is consistently accurate across varied clinical contexts can become dependable. The gap between those two states is where much of the current hesitation sits.
Explainability Is Becoming a Clinical Requirement
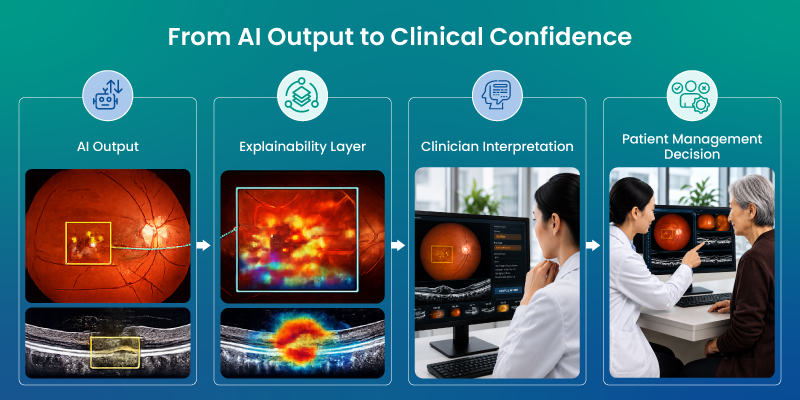
Ophthalmic decision-making is not only about identifying an abnormality. It is about understanding why it matters.
That is why explainability is becoming central to AI trust. Clinicians need to understand how an AI system reached its conclusion, which visual features influenced the result, and whether the output aligns with the broader clinical picture.
The need for transparent, explainable AI extends well beyond ophthalmology, with similar challenges shaping the adoption of AI in Mental Health, where clinician trust and accountable decision-making remain equally important.
Without this, AI can feel like a black box. Even when its output is correct, the clinician may still hesitate because the reasoning is not visible enough to support a confident decision.
This is especially important in glaucoma progression, retinal disease management, and treatment-defining decisions, where small changes in interpretation can alter follow-up intervals, referral urgency, or treatment planning.
In real practice, explainability is not a technical extra. It is part of clinical accountability.
Trust Changes as Clinical Risk Increases
One of the clearest patterns in the draft is that AI trust is contextual. Clinicians are more comfortable with AI in screening, early detection, and workflow-support scenarios. Caution increases when AI moves closer to complex diagnosis, high-risk interpretation, or treatment-defining decisions.
This is a rational adoption pattern.
If AI misses a screening flag, the system risk is different from an AI output influencing treatment escalation in a complex glaucoma patient or management change in retinal disease. As clinical risk rises, clinicians need higher confidence, stronger validation, clearer reasoning, and defined responsibility.
This is why AI adoption in ophthalmology is likely to remain layered. It may become routine in image triage or screening before it becomes trusted in final diagnosis or independent patient management decisions.
The technology may expand quickly. Trust will move more slowly.
Workflow Integration Will Decide Practical Value
AI does not create value simply by producing an output. It creates value when that output fits the clinical workflow.
If clinicians must repeatedly cross-check results, manually reconcile AI findings with existing systems, or spend extra time explaining uncertain outputs, AI may add work instead of reducing it.
This is a major real-world integration issue. For AI to become a dependable layer in ophthalmic care, it must align with imaging systems, documentation practices, referral pathways, and clinician review processes. The more seamlessly it fits, the more likely it is to support care rather than interrupt it.
This level of interoperability is also a defining characteristic of the modern Smart Hospital, where connected technologies work together to improve clinical efficiency and decision-making.
The MDForLives insight points to a larger truth: AI trust is not built only through better algorithms. It is built through better clinical integration.
What Will Move AI From Useful to Trusted?
The next phase of AI in ophthalmology will likely depend on four factors.
First, real-world validation across diverse patient populations, devices, image qualities, and practice settings. Second, consistent performance in everyday clinical variability. Third, explainability that helps clinicians understand and defend outputs. Fourth, workflow integration that reduces friction rather than adding verification burden.
These are not abstract requirements. They are the conditions under which ophthalmologists can move from using AI to relying on it.
Closing Perspective
AI in ophthalmic imaging has already entered clinical practice. It is helping clinicians manage image-heavy workflows, detect disease earlier, and support interpretation in selected settings.
But the MDForLives findings show that adoption and trust are not the same.
A majority of clinicians report regular use of AI, yet fewer report full confidence in its outputs. Concerns around consistency, over-reliance, explainability, and workflow fit continue to shape how far clinicians are willing to let AI influence decisions.
This does not weaken the case for AI in ophthalmology. It makes the next challenge clearer.
The future will not be defined only by whether AI can detect more. It will be defined by whether clinicians can trust AI enough to act with confidence when the stakes are higher.
That emphasis on timely, confident clinical decisions is equally important in conditions such as sudden cardiac death in athletes, where early recognition and intervention can be lifesaving.
FAQs
How is AI currently used in ophthalmology?
AI is commonly used in ophthalmic imaging workflows such as retinal screening, OCT interpretation, diabetic retinopathy detection, glaucoma assessment, and reporting support.
Why is AI adoption rising in ophthalmic imaging?
Ophthalmology is image-rich and data-driven, making it well suited for AI tools that support pattern recognition, screening efficiency, and earlier disease detection.
Why is clinical trust in ophthalmic AI still limited?
Clinicians still need stronger confidence in real-world consistency, explainability, workflow integration, and performance across variable imaging conditions and patient presentations.
What does explainability mean in ophthalmic AI?
Explainability means clinicians can understand why an AI system produced a specific output, including which imaging features or patterns influenced the result.
Will AI replace ophthalmologists in diagnosis?
The current real-world pattern suggests AI is more likely to support ophthalmologists than replace them. Clinicians continue to retain responsibility for interpretation, patient management, and high-risk decisions.
What will make AI more trusted in ophthalmology?
Greater trust will likely depend on real-world validation, consistent performance, transparent outputs, clear medico-legal responsibility, and integration into everyday clinical workflows.

MDForLives is a global healthcare intelligence platform where real-world perspectives are transformed into validated insights. We bring together diverse healthcare experiences to discover, share, and shape the future of healthcare through data-backed understanding.



