What should an oncologist do when a blood test suggests recurrence, but the scan still shows nothing?
That question is becoming one of the most important clinical tensions in modern oncology.
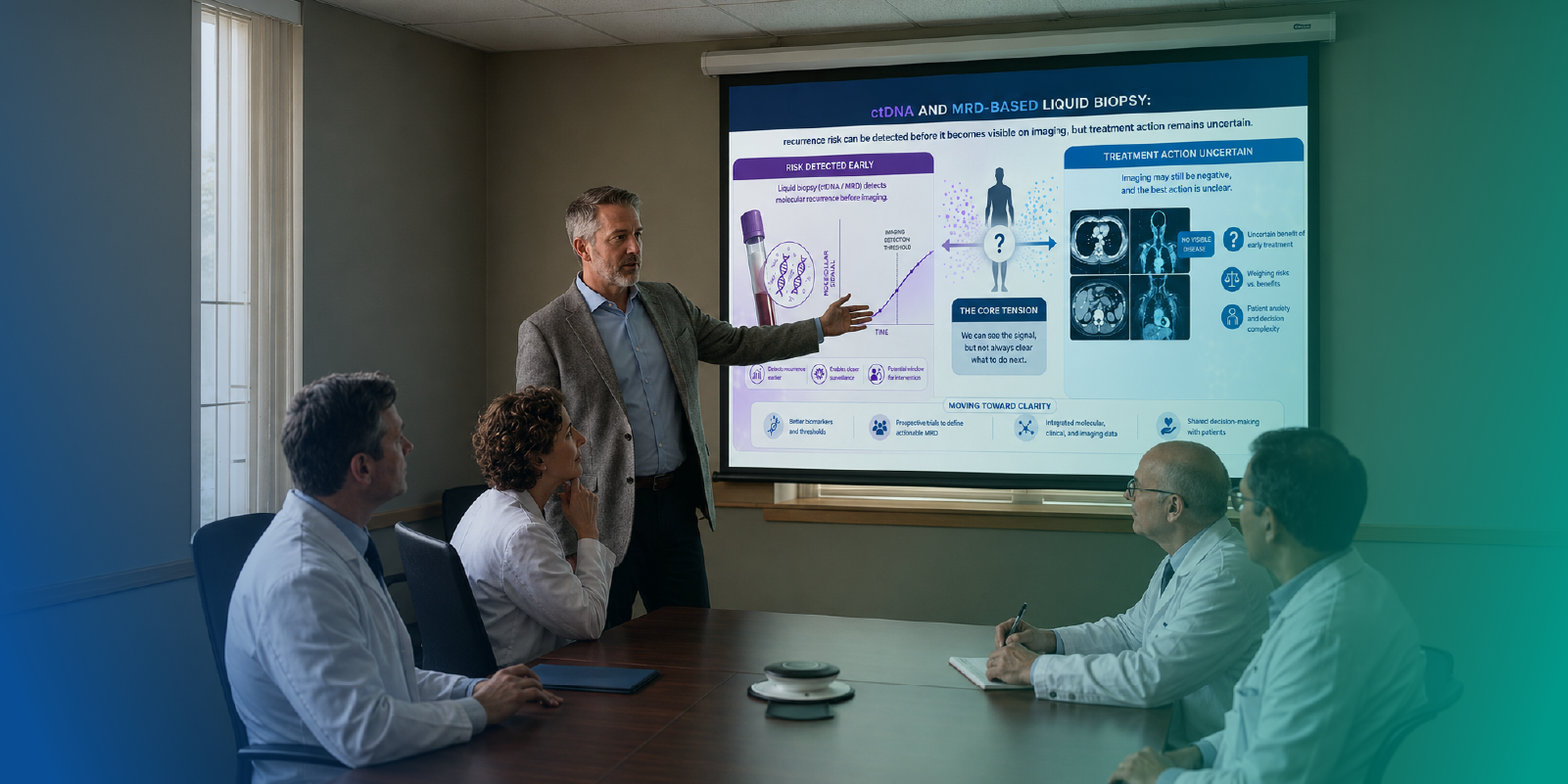
Liquid biopsy, particularly circulating tumor DNA or ctDNA-based MRD testing, is changing what clinicians can see after curative-intent treatment. It can detect molecular signs of residual disease before recurrence becomes visible on imaging. In theory, that creates a powerful window: identify relapse earlier, intervene sooner, and potentially reshape surveillance or adjuvant treatment planning.
But in real practice, earlier detection creates a harder question.
Can you act before you see?
The MDForLives insight reflects this exact gap. Across a global sample of oncologists, 58.1% report actively using ctDNA in practice. Nearly half, 48.4%, identify early detection of recurrence before imaging as its greatest benefit. Yet only 29.0% say ctDNA is already influencing treatment decisions in select cases.
The pattern is clear: detection is ahead of decision.
ctDNA Has Moved Into Practice
The first important signal is adoption. When 58.1% of oncologists report actively using ctDNA, liquid biopsy is no longer sitting outside routine oncology conversations. It has entered clinical workflows, especially in surveillance, post-treatment monitoring, and risk stratification.
This matters because the debate is no longer about whether ctDNA is scientifically interesting. Most oncologists already recognize its potential value.
The bigger question is where it becomes actionable.
48.4% see early recurrence detection before imaging as the greatest benefit. That is a strong endorsement of ctDNA’s clinical promise. Imaging remains central to oncology, but molecular detection is creating a new layer of visibility, one that may appear before radiologic recurrence.
That changes the timing of uncertainty.
Earlier Detection Does Not Automatically Mean Earlier Treatment
The clinical value of ctDNA is easy to understand. The clinical response is harder.
Only 29.0% say ctDNA is already influencing treatment decisions in select cases, while 45.2% say it remains promising but still requires more evidence before action.
This is not a lack of awareness. It is a hesitation at the point of consequence.
Acting on ctDNA can mean escalating treatment, intensifying surveillance, enrolling a patient in a trial, or changing the follow-up pathway before recurrence is visible. Each of those decisions carries implications for toxicity, cost, anxiety, and patient quality of life.
The oncologist is not simply asking, “Is the result positive?”
They are asking, “Will acting on this result improve the patient’s outcome?”
This question is especially relevant in breast cancer recurrence, where detecting relapse earlier is valuable only when it leads to more informed and effective treatment decisions.
That distinction defines the current state of ctDNA-guided oncology.
Trust Is Conditional When Imaging Is Negative
The data shows that when a patient has positive ctDNA but negative imaging, only 22.6% of oncologists are very likely to trust the result. A larger share, 41.9%, are only somewhat likely.
This finding captures the transitional mindset around liquid biopsy.
Oncologists recognize the signal. They may not yet trust it enough to change treatment in every case.
A similar balance between improved detection and clinical confidence is also being seen in AI in endoscopy, where clinicians continue to evaluate how AI findings should influence patient care.
A positive ctDNA result can feel clinically meaningful, but if imaging remains negative, the oncologist faces a difficult interpretive gap. Is this molecular relapse that will become visible soon? Is it a signal that requires urgent escalation? Could it lead to overtreatment? Is the assay reproducible enough in this tumor type and setting?
In oncology, confidence is not only about test sensitivity. It is about what follows the test.
The Barrier Is Actionability, Not Curiosity
The biggest barriers are decision-making barriers, not interest barriers. 38.7% cite lack of clear guidelines on what to do next, while 29.0% question whether acting on ctDNA actually improves outcomes.
That is the heart of the issue.
ctDNA can generate earlier information. But oncology needs evidence that earlier action changes meaningful endpoints, such as recurrence-free survival, progression-free survival, overall survival, or avoidance of unnecessary treatment.
Without that, the test may create knowledge without a clear pathway.
This same pattern can also be seen in ADCs in Oncology When Clinical Promise Moves Faster Than Practice Confidence, where promising therapies are moving into practice as supporting evidence continues to grow.
For clinicians, that can be uncomfortable. A positive result may make everyone feel that something should be done. But if the best action is unclear, early detection can become an ethical and practical dilemma.
Escalation Feels More Ready Than De-Escalation
The Questionnaire explores comfort with both escalation and de-escalation. That distinction is important.
In practice, ctDNA may feel easier to use for escalation than de-escalation. A positive result after curative-intent treatment can support the idea that residual disease may exist. But using a negative result to reduce therapy may require a different level of confidence, especially when the consequence is potentially undertreating a patient who could recur.
The data identifies adjuvant therapy escalation and early surveillance as the most ready applications, at 38.7% and 35.5% respectively.
That pattern suggests oncologists may be more comfortable using ctDNA as a risk signal than as a standalone treatment selector.
In other words, ctDNA is influential. It is not always decisive.
The Central Dilemma: Overtreating vs Missing the Window
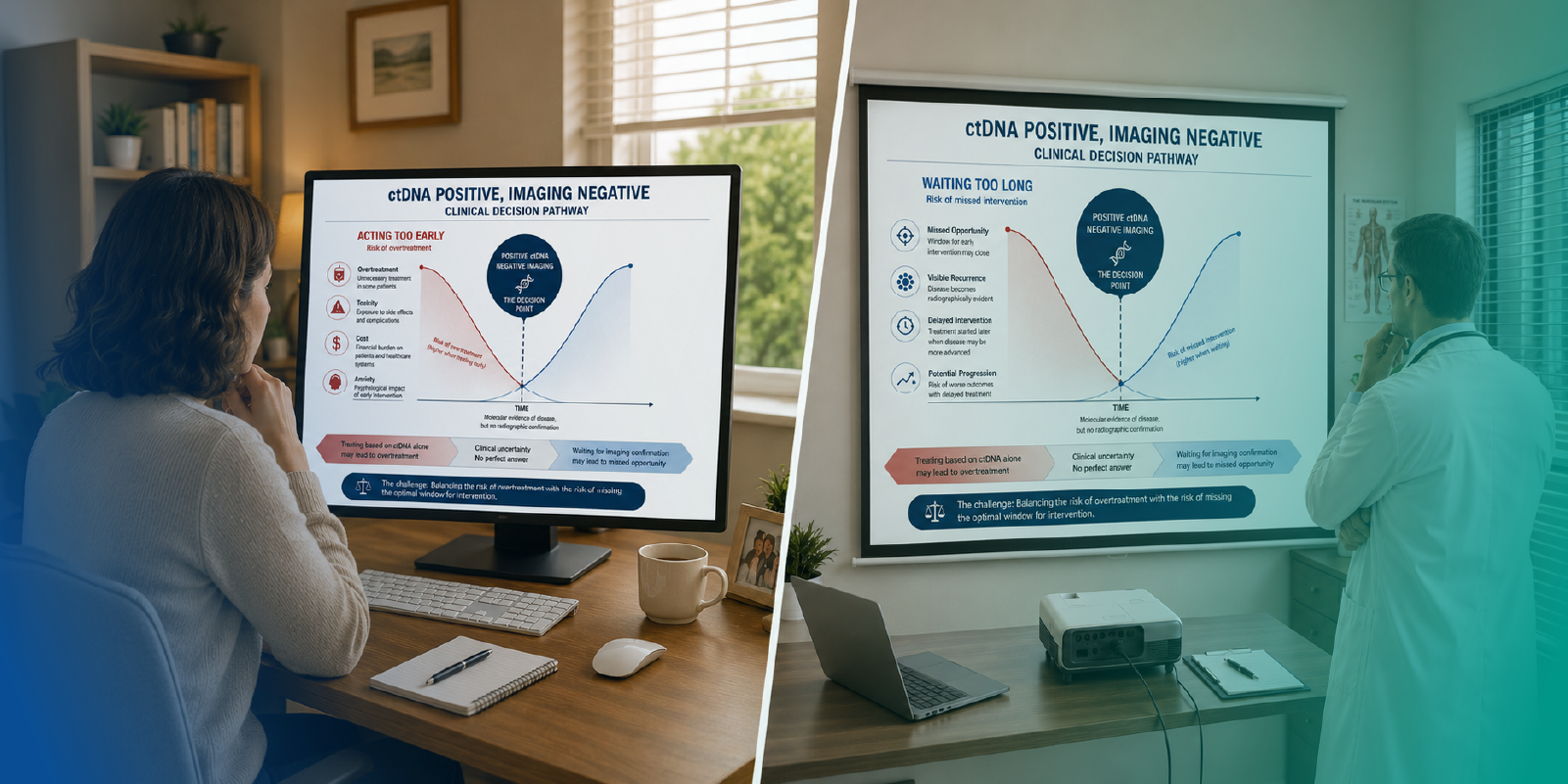
The most defining concern is overtreatment. 35.5% say their main concern is over-treating patients without proven benefit, followed by uncertainty around treatment timing and selection.
This shows why early detection is not automatically simple.
If clinicians act too early, some patients may receive unnecessary treatment, added toxicity, cost, and anxiety. If they wait too long, they may miss the chance to intervene before visible relapse.
This is the paradox of molecular recurrence.
The technology moves the alarm earlier. The evidence has to tell clinicians what to do with the alarm.
What Would Make ctDNA Truly Actionable?
45.2% want randomized trials demonstrating improved outcomes. Another 35.5% want clearer clinical guidelines.
That is a practical roadmap for confidence.
A similar transition is taking place with PSMA PET imaging for prostate cancer, where growing diagnostic accuracy is strengthening confidence in personalized treatment planning and disease assessment.
Oncologists are not asking for more excitement around ctDNA. They are asking for prospective evidence, tumor-specific validation, assay reliability, reimbursement clarity, and action pathways after a positive result.
This is where the next phase of liquid biopsy will be decided. The field has moved from capability to validation. The next step is standardization.
Closing Perspective
Liquid biopsy has already changed what oncology can detect.
It has not yet fully changed what oncology is willing to do.
The MDForLives findings reveal a clear pattern: oncologists are using ctDNA, they see its strongest value in detecting recurrence before imaging, and they expect it to become more important. But when the decision involves acting before visible recurrence, confidence becomes conditional.
The real question is no longer whether ctDNA can detect risk earlier.
It is whether oncology can build the evidence, guidelines, and treatment pathways needed to act on that risk responsibly.
The same transition is taking place in AI in ophthalmic imaging, where stronger evidence and clinical trust remain essential for translating innovation into everyday practice.
Because in cancer care, seeing earlier matters.
But deciding earlier is what will define the next era.
FAQs
What is ctDNA in oncology?
ctDNA, or circulating tumor DNA, refers to tumor-derived DNA fragments found in the bloodstream. It can be studied through liquid biopsy to support molecular profiling, monitoring, recurrence assessment, and MRD evaluation in selected settings.
What is MRD testing in solid tumors?
MRD, or molecular residual disease, refers to cancer-related molecular signals that may remain after treatment even when disease is not visible through conventional imaging.
Why is ctDNA important for recurrence monitoring?
ctDNA may detect molecular recurrence before recurrence appears on imaging, potentially giving clinicians an earlier signal of relapse risk.
Why are oncologists cautious about acting on ctDNA results?
The main concerns are lack of clear guidelines, uncertainty about whether acting improves outcomes, false positive or false negative concerns, and lack of defined treatment pathways after a positive result.
Is ctDNA ready to guide treatment decisions routinely?
It is increasingly used in selected settings, but many oncologists still want stronger prospective evidence and clearer guidelines before using it routinely to escalate or de-escalate treatment.
What would increase confidence in ctDNA-guided decisions?
Randomized trials showing improved outcomes, tumor-specific validation, assay standardization, clearer guideline recommendations, access support, and defined action pathways would increase confidence.

MDForLives is a global healthcare intelligence platform where real-world perspectives are transformed into validated insights. We bring together diverse healthcare experiences to discover, share, and shape the future of healthcare through data-backed understanding.